









Barrett’s Oesophagus
An Important Consideration for all Reflux Patients
Barrett’s Oesophagus
Barrett’s Oesophagus is named after a famous British surgeon, Norman Barrett. It describes a condition associated with Reflux Disease in which the normal cells lining the bottom of the oesophagus are replaced by abnormal cells. In turn, these ‘abnormal’ cells are associated with an increased risk of developing oesophageal cancer.
The precise number of people in the general population with Barrett’s isn’t known. However, 20–30% of the adult population has reflux disease (GORD), and of these, 5–10% will have Barrett’s.
Of all those people referred for an endoscopy by their GP, studies suggest that as many as 1 in 5 will be diagnosed with Barrett’s. Naturally, these are concerning figures, and the risk means that it is of paramount importance that those who have suffered from reflux symptoms over a long period of time undergo a gastroscopy to observe any cell damage this may have done.
To explain Barrett’s Oesophagus, we must get rather technical; hence this is a long and detailed leaflet. It is such an important subject and of concern to so many people that we meet in a clinic that we have decided to provide a very comprehensive guide. We’ve tried to write it in such a way that it is easy to follow.
The Oesophagus
Food and liquids pass from the throat into the oesophagus when we swallow them. This is essentially a muscular tube that passes through the chest cavity behind the heart and then empties into the stomach, where the digestive process starts. The gut is lined by cells, a little bit like the wallpaper lines the walls of a room. This is called the ‘mucosa’. Since different parts of the gut perform various functions, these cells vary along their length to reflect these functions. In the oesophagus, these cells merely protect the underlying muscle layer and are flat, pale, and oriented in layers, very much like those in the skin. This is called the stratified epithelium. However, the stomach has many other functions, including secreting mucus, acid and enzymes, and here, the cells are quite different, being more square, red in colour and organised as ‘columns’. This is called the columnar epithelium.
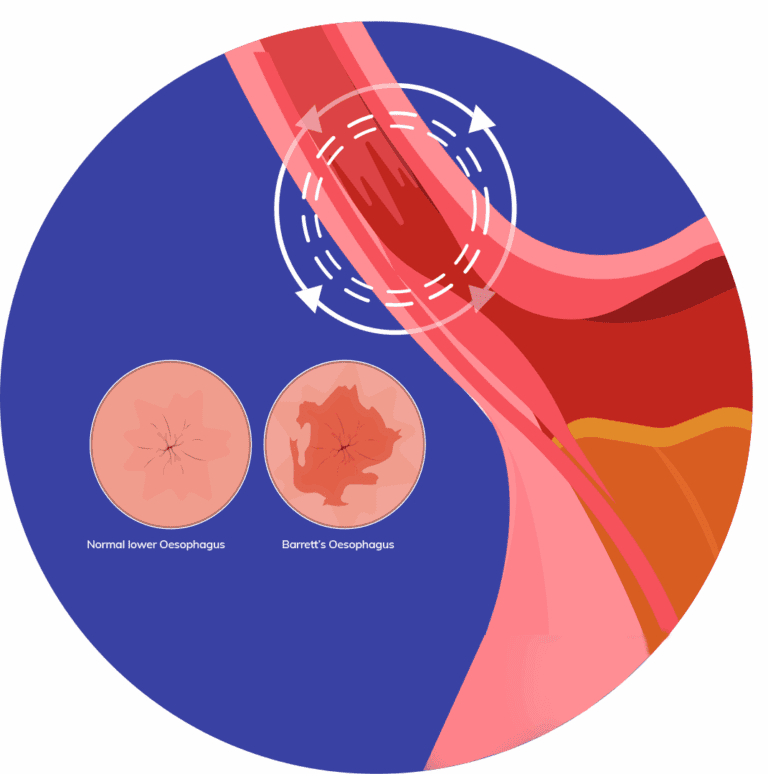
Observing Barrett’s Oesophagus
In Barrett’s, the cells at the bottom of the oesophagus change from the stratified type to resemble columnar epithelium. The appearance, therefore, changes from a pale colour to a reddish ‘salmon pink’ and is sometimes called a ‘columnar-lined oesophagus’.
Barrett’s is also known as ‘columnar metaplasia’. Metaplasia is a condition in which one adult cell replaces another. In Barrett’s, columnar cells replace stratified cells, hence columnar metaplasia.
Strictly speaking, Barrett’s is divided into ‘long segment’ and ‘short segment’ diseases. A ‘short segment’ is defined as abnormal cells that extend no more than 3 cm from the top of the stomach, and a ‘long segment’ is defined as abnormal cells that extend 3 cm or more from the top of the stomach. This distinction helps doctors stratify risk, as the longer the segment of Barrett’s, the more abnormal cells it will contain and the more likely it may progress to cancer. Barrett’s short segment is about three times more common than Barrett’s long segment.
What Causes Barrett’s Oesophagus?
Barrett’s oesophagus is caused by the repeated inflammation of the oesophagus that arises from gastro-oesophageal reflux disease (GORD). Normally, the valve mechanism at the bottom of the oesophagus, known as the lower oesophageal sphincter (LOS), prevents excessive reflux of acid and other stomach contents into the oesophagus. When this valve fails, the cells lining the bottom of the oesophagus are exposed to hydrochloric acid, pepsin, bile salts and other substances that are usually kept within the stomach. This can cause inflammation, and in response to repeated episodes of inflammation, the cells change (undergo metaplasia) from stratified to columnar epithelium.
Both GORD and Barrett’s can run in families, but there is currently no specific genetic test that can predict outcomes. Barrett’s is also associated with obesity, especially in middle-aged men, and smoking.
It’s worth noting that some patients who often develop Barrett’s do not suffer typical reflux symptoms and are only diagnosed with Barrett’s when they start to experience symptoms from other conditions, including oesophageal cancer.
It’s also worth noting that symptoms of reflux very often improve as Barrett’s progresses. This does not indicate that reflux has resolved or that there is no longer inflammation occurring, but it probably reflects a change in the nervous system’s perception of the symptoms caused by reflux.
Is Barrett’s Oesophagus Dangerous?
Once patients are diagnosed with Barrett’s, it’s quite usual that they become very concerned. This is because Barrett’s can be a premalignant condition. The most common type of oesophageal cancer in the UK and Europe occurs at the junction of the stomach and oesophagus and is associated with Barrett’s, known as adenocarcinoma. This type of cancer has been one of the fastest growing malignancies in terms of the number of people diagnosed over the past 30 years. However, it’s important to remember that while Barrett’s is common, oesophageal cancer is rare, and most people with Barrett’s will not develop cancer.
There are many confusing terms associated with Barrett’s and its stepwise development into cancer. Barrett’s itself is otherwise known as ‘columnar metaplasia’ because the normal cells lining the bottom of the oesophagus have changed, or ‘undergone metaplasia’, from stratified to columnar epithelium. This lining is also known as the mucosa. In response to repeated inflammation, these cells can then change further, a process called ‘dysplasia’, which describes the development of abnormal tissue. In fact, dysplasia is further divided according to severity into ‘low grade’ and ‘high grade’. This signifies a significant increase in the risk of the cells progressing to the final step on the path to the development of cancer (carcinoma), ‘neoplasia’, or new tissue. Again, there are effectively two stages in the development of carcinoma.
In the first, the cancerous cells are confined to the mucosa. This is called intra-mucosal (or sometimes intra-epithelial) carcinoma. The final step in the development of cancer is when the cells spread through the other layers of the wall of the oesophagus and have therefore become invasive carcinoma. So, Barrett’s is a premalignant condition, and it undoubtedly confers an increased risk of developing adenocarcinoma of the oesophagus. The size of this risk remains in dispute but is probably between 30 and 125 times the average population. Nonetheless, cancer of the oesophagus remains relatively uncommon, so most people diagnosed with Barrett’s will not progress to develop cancer. The size of the risk varies to some extent, but overall, it is about 0.5% per year, and only one in twenty people with Barrett’s will develop cancer. Once dysplasia develops, however, the risk per year increases significantly. The risk of high-grade dysplasia progressing to cancer is at least 10% per year.
Frequently Asked Questions
This is called ‘screening’, and there is no evidence that it is justified in the general population. However, if you have reflux symptoms and specific risk factors for the development of oesophageal cancer, your specialist may recommend an endoscopy.
Barrett’s is a premalignant condition, and in a small number of patients, it will develop into cancer. This is the last stage in a progression through several stages, during which the damage to the DNA in the cells at the bottom of the oesophagus gradually becomes more and more severe. Having been diagnosed with Barrett’s, there is, therefore, an argument in favour of performing regular ‘surveillance’ endoscopies with further biopsies to check for progression. There is evidence that this can identify changes at an early stage and improve survival.
However, exactly how often an endoscopy should be performed will be dependent on several factors, including the length of Barrett’s segment and the findings from previous endoscopies. Endoscopies are usually performed every 2–5 years, but in some cases—for example, when dysplasia is discovered—they are performed more frequently. It would help if you discussed this with the specialist who is looking after you.
Uncomplicated Barrett’s:
Unless dysplasia or cancer develops, current evidence suggests that intervention is not indicated. In other words, the risks of removing Barrett’s cells are more significant than the likely benefit and should therefore be avoided.
However, your specialist will discuss the options for drug treatment in particular, the use of high-dose Proton Pump Inhibitors (PPIS) and aspirin.
Complicated Barrett’s:
Once dysplasia or cancer develops, further treatment becomes necessary. The precise type of treatment will depend upon the nature of the abnormalities, and there are several options now available:
- Photodynamic therapy (PDT): Abnormal cells in Barrett’s segment are destroyed by laser light. It has largely been replaced by radiofrequency ablation.
- Endoscopic radiofrequency ablation (RFA): A small coil is guided towards the abnormal section of the oesophagus. This emits heat, which destroys abnormal cells, which are subsequently replaced by normal cells.
- Argon plasma coagulation: A jet of argon gas is directed at abnormal cells. An electric current is transmitted by the gas, which then burns the cells.
- Endoscopic mucosal resection (EMR): Barrett’s cells, in the absence of invasive cancer, are confined to the layer of cells that lines the oesophagus (the mucosa). This can be lifted from the underlying muscle layers in the same way that wallpaper is removed from the walls of a room. The procedure is performed endoscopically using special instruments that enable
the resection of the abnormal tissue. Even early cancers can be removed using this technique, avoiding major surgery.
Barrett’s is caused by Gastro Oesophageal Reflux Disease (GORD). Reflux causes chronic inflammation at the bottom of the oesophagus, and the major contributor to this is acid from the stomach. This is why antacid drugs are the mainstay of treatment for the symptoms caused by reflux. The most potent antacids are PPIs (Proton Pump Inhibitors) such as Omeprazole and Nexium. PPIs have now been shown to improve survival benefits in patients with Barrett’s Oesophagus. An extensive scientific study called the AspECT trial published in 2018 demonstrated that patients who took high doses of PPIs enjoyed a survival benefit over those who did not. There was a further benefit if aspirin was added. However, PPIs are associated with other conditions, in particular with Small Intestinal Bacterial Overgrowth (SIBO), in which there is abnormal colonisation of the gut by bacteria. Consequently, having been diagnosed with Barrett’s, we would advise that you discuss the benefits and risks of treatment with your specialist.
Barrett’s is a precursor to the most common type of oesophageal cancer in the UK. Adenocarcinoma, which develops at the bottom of the oesophagus at the junction with the stomach, is almost always associated with Barrett’s Oesophagus. The ‘metaplasia’ that defines Barrett’s occurs as a consequence of reflux and probably as a healing response to the inflammation that occurs when the oesophagus is bathed in acid, bile, pepsin and other components of gastric juice. Gastric acid can cause DNA damage in Barrett’s cells, cause the proliferation of Barrett’s, and also cause the secretion of cytokines, the chemical messengers associated with inflammation. There is clear evidence from clinical trials that PPIs improve survival in patients with Barrett’s. There is also evidence that it’s not just acid that causes a problem—bile salts also seem to cause the release of cytokines and may even be more chemically active in low-acid environments, for instance, when patients are taking PPIs. So, if reflux causes Barrett’s and Barrett’s is associated with cancer, surely an operation that stops reflux will also prevent cancer from developing? It’s quite possible that this is the case.
In fact, a study published in 2019 suggested that Barrett’s regressed following LINX® implantation, and there is other ‘observational’ evidence that successful anti-reflux surgery reduces the development of both dysplasia (the precursor to cancer) and cancer itself. However, while hypothetically, the theory is very appealing, we don’t actually have definite proof from a prospective scientific study that this is the case. Why not?
Firstly, most people with Barrett’s don’t develop cancer. The risk is about 0.5% per year, so it would require following many thousands of people over many years to see a difference between those who had surgery and those who didn’t. Secondly, it’s well known that PPIs improve survival in Barrett’s Oesophagus, and any study would have to compare two groups of patients, one taking PPIs and the other having surgery. So, it would be tough to construct a scientific study comparing outcomes in a disease that takes many years to develop. It’s unlikely that such a study will ever be performed. So, the answer to the question is that, as things stand, there is no evidence that having an anti-reflux operation will stop the development of cancer any more than PPIs.
However, the bigger question is: what should people who have persistent symptoms do despite PPIs if they also have Barrett’s and can’t or don’t want to take PPIs? This question applies to many people, as 20–30% of those who take PPIs to control reflux still suffer regular symptoms, and an increasing number of patients do not want to take these powerful drugs indefinitely. The answer again is unknown, but it seems sensible to consider that surgery may well confer the additional benefit of reducing the risk of developing cancer in addition to abolishing reflux symptoms.
For these reasons, some people may believe that the possibility of preventing the development of cancer is another reason to consider surgery.

